|
! Avertissement -
Warning
!
|
|
Si vous arrivez
directement sur cette page sachez que ce travail est un
rapport d'étudiant(e)s et doit être pris comme
tel. Il peut donc comporter des imperfections ou des
imprécisions que le lecteur doit admettre et donc
supporter. Nous ne faisons aucun usage commercial et la
duplication est libre. Si vous avez des raisons de contester
ce droit d'usage, merci
de nous en faire
part. L'objectif
de la présentation sur le Web est de permettre
l'accès à l'information et d'augmenter ainsi
les échanges professionnels. En cas d'usage du
document, n'oubliez pas de le citer comme source
bibliographique. Bonne lecture...
You are welcome to use
this webpage which presents students' reports, studies or
thesies. Nobody is perfect and it is possible to find some
mistakes in this document. We apologize if you are shocked
or disappointed by some of them and very grateful if you
could contact
us in order to
improve our works. The content of this website is free and
you can duplicate it as you want! But please, observe the
Internet Exchange Ethic and do not forget to cite this works
on yours !.. Thanks and enjoy it...
|
Université
de Technologie de Compiègne
- Compiègne
University of Technology
|
Réference
à rappeler : Planification
Stratégique et Amélioration Continue en
Enseignement Supérieur, Recherche et Hôpital,
Mastère NQCE session professionnelle,
UW-Madison, CQPI, 2000, p
61,http://www.utc.fr/~farges/Qualite/Q_Madison/Madison.htm
Reference to
make: Strategic Planning & Continuous Improvement in
Higher Education, Research & Hospitals,
Mastère NQCE professional session, UW-Madison,
CQPI, 2000, p 61,
http://www.utc.fr/~farges/Qualite/Q_Madison/Madison.htm
|
Strategic
Planning
& Continuous
Improvement
in Higher
Education,
Research
& Hospitals
"Experiences
at
UW-Madison
and Transfer
to the French
Context"
|
- Etude réalisée de mars à mai
2000 à l'Université de Madison - Wisconsin
- USA par :
- Working place UW-Madison, from
March up to May 2000, report written by :
-

|
Gilbert
FARGES, enseignant-chercheur en technologies
biomédicales à l'Université
de Compiègne, responsable et animateur de
formations d'ingénieurs et de techniciens
supérieurs biomédicaux
hospitaliers. Mes activités
d'enseignement et de recherche m'amène
naturellement à m'intéresser aux
développements des démarches
qualité dans l'enseignement
supérieur.
- Gilbert
Farges, teacher and researcher in
biomedical and hospital clinical engineering
at the University of Technology of
Compiègne. Since a long time, I am
very interested to develop and implement
quality management in Higher Education,
Scientific Research and
Hospitals.
-
-
UTC,
BP 20.529, 60205 Compiègne Cedex,
France, Tel : [33] (0)3 44 23 44 58,
Fax : [33] (0)3 44 20 48
13
- E-mail :
gilbert.farges@utc.fr
URL
: http://www.utc.fr/~farges
|
|
Résumé :
Cette étude présente la
découverte du management par la qualité
totale en Université et Hôpital: la
Planification Stratégique et l'Amélioration
Continue sont utilisées quotidiennement dans de
nombreux Départements ou Services de
l'Université du Wisconsin- Madison aux USA. Le
modèle de management et son application sont
présentés, ainsi que la méthode pour
introduire progressivement la culture qualité
auprès de l'ensemble du personnel universitaire,
à tous les niveaux et aussi bien dans les secteurs
de l'enseignement supérieur, que celui de la
recherche scientifique ou de l'hôpital.
L'application au contexte français est
proposée à travers deux projets
intéressant l'université, l'un en
organisation de la recherche, l'autre en formation
continue professionnelle de haut niveau.
Mots-clefs : Management de la
Qualité, Planification Stratégique,
Amélioration Continue, Enseignement
Supérieur, Recherche Scientifique,
Hôpital
|
Summary :
Discovery of the total
quality nmanagement principles applied at the University
and Hospital: Strategic Planning and Continuous
Improvement are daily used in a lot of departments and
services of the University of Wisconsin-Madison. This
study presents the applied management model and how the
quality culture is progressively introduced towards
faculty, instructional and staff members as well as in
teaching and learning, scientific research and hospital
areas. Transfer of such management methods is proposed
about two university projects in research organization
and in continuing higher education.
Keywords : Quality
Management, Strategic Planning, Continuous Improvement,
Higher Education, Research, Hospitals
|

Acknowledgments Aims
of the project
Chapter 1: Quality
Management at UW-Madison
A)
About University of Wisconsin- Madison
B)
Strategic Planning and Continuous
Improvement
C)
Operational organization around Quality at
UW-Madison
Chapter 2: Quality
Teaching & Learning Experiences at
UW-Madison
A)
UW-Madison Teaching Academy
B)
Creating a Collaborative Academic Environment (CCAE)
Chapter 3: Research
& Quality Management Experiences at
UW-Madison
A)
Continuous Improvement at
RSP
B)
Biomedical Engineering Department
Chapter 4:
University Hospital & Quality Management Experiences
A) About
University of Wisconsin Hospital and Clinics
B)
Quality Improvement Department
C)
Medical Physics Department
D)
Clinical Engineering Department
Chapter 5 :
Synthesis and transfer possibility to the French
context
A) Quality
in Research at UTC
B)
Quality in Hospitals
Conclusion
Bibliography
Appendix
A: OQI
: Office for Quality Improvement
B: CQPI :
Center for Quality & Productivity
Improvement
C:
The 14 points of Deming’s quality
management
D: Quality
websites
I thank the UW-Madison teams, researchers, members,
staff, students, and especially CQPI, for their open-mindedness,
confidence and friendly help and collaboration during the stay and
I will enjoy any future scientific collaboration:
- François Sainfort, Ph.D., Director of CQPI for his
invitation to share the great quality experiences at
UW-Madison,
- George Box, Ph.D. and Professor Emeritus, for sharing his
great scientific knowledge during CQPI seminars,
- Pascale Carayon, Ph.D. and Peter Hoonakker for their very
friendly welcome and interest,
- Marlene Beilman for her useful help to plan and manage my stay
(before, during and maybe after ?),
- Murat Kulahci, Ph.D. & Ernseto Barios for their friendly
advises,
- Mary Ellen Hagenauer, Kassy Hilber, John Tyssedal, Ph.D. &
Ben-Tzion Karsh, Ph.D. for their daily kindness,
- Maury Cotter for her helpful meetings despite an overbooked
agenda !
- Lois Brako, Ph.D., for her very helpful and documented meeting
to understand quality at RSP,
- Katherine Sanders, Ph.D. and Christopher Carlson-Dakes for
their friendly meeting about the very impressive goal to create
collaborative environment in teaching, learning and research in
order to serve the Vision of the University,
- Ann Zanzig and John M. Elliott for their very understandable
workshop about strategic planning and continuous improvement,
- John Webster, Ph.D. and Nancy Webster for their kindly welcome
and help during my stay,
- Nancy Speck, Jack Bowhan & Carl Selbo for their welcome,
helpful meetings and documentation and maybe future
collaboration?
- Bruce Thomadsen, Ph.D. & Frank Narallo, Ph.D., for their
useful meetings, advises and interest about my project,
- William Bloomer for his discussion about clinical
engineering.
back to Contents
Like teacher, researcher and biomedical engineer, I always have been
interested by techniques and methods to manage technology, innovation
and organization.
In France, a recent law1 requests
quality in public or private hospitals and has created a strong
movement in favor of quality approaches and improvement methods into
the organizations.
In the field of the higher engineering education and research, a
recent
study2 also shows that
European Union recommends to develop assurance quality management
methods in Colleges and Universities in all European countries, at
all levels in the teaching area and even if possible in
research3 .
In order to be able to efficiently teach, understand, research, plan
and manage quality in my professional field, I decided one year ago
to attend a higher engineering diploma in quality. It has been not
very easy to plan and do it in the same time of my busy job. But with
a strong and well planned organization, a comprehensive family (and
wife), friendly colleagues, in Spring 1999 I could attend the first
theoretical part of the training.
Spring 2000 is the planned period for the second part of the course:
the practical and professional training which I wanted in a well
experimented university area, in order to understand the keys to
successfully manage a quality development. I am very grateful to the
Center of Quality and Productivity Improvement of the University of
Wisconsin-Madison, and especially to its Director François
Sainfort, to share with me its experience and knowledge.
This CQPI stay is the first half part of my practical training
session, because I will go to Montreal University for the second and
last part, more focused about quality management for hospitals.
back to Contents
Chapter 1
Quality Management at University of
Wisconsin-Madison
|
A) About University
of Wisconsin-Madison4
:
(source :
http://www.news.wisc.edu/welcome/mission.html)
Madison (200,000 inhabitants) is the capital city of the state of the
Wisconsin (5,000,000 inhabitants) (figure 01). The median age of the
Madison population is 33 and almost 70% to 75% of Madisonian are
under 445 .


Fig 01: Geographic situation of Madison (left) and
the Wisconsin State Capitol (right)
“Entrepreneur
Magazine”6 ranks
Madison as one of the top 5 cities in the USA in which to start a
business. More than 350 firms in the Greater Madison Area are defined
as high-tech: 25% of these firms are in manufacturing and service
sector (biotechnology, medical/biomedical research,
micro-electronics, pharmaceutical, contract research and development,
software...)
Research activity on the University of Wisconsin-Madison campus is a
major stimulus for growth in the area's economy. Over the last five
years the number of high-tech firms has grown 20%. The University of
Wisconsin-Madison ranks in the top echelons of American research
universities. UW-Madison annually receives total research funding
exceeding $363 million. According to the latest figures available
from the National Science Foundation, this makes the University of
Wisconsin-Madison the third largest funded research university in the
USA.
back to Contents
Founded in 1849, the university is a public, land-grant
institution that provides on a single campus a complete spectrum of
liberal arts studies, professional programs and student activities.
UW-Madison academic reputation has been rated among the top 10 in
many areas of study since 1910.


Fig 02: Some views of the campus of the
UW-Madison
The primary purpose of the University of Wisconsin-Madison is to
provide a learning environment in which faculty, staff and students
can discover, examine critically, preserve and transmit the
knowledge, wisdom and values that will help ensure the survival of
this and future generations and improve the quality of life for all.
The university seeks to help students to develop an understanding and
appreciation for the complex cultural and physical worlds in which
they live and to realize their highest potential of intellectual,
physical and human development.
Some statistics (1999):
Students: 40,000
Costs/year: $11,000 (non-resident: $20,000) (includes room, books,
supplies...)
Alumni: 320,000
Staff: 18,000 (Faculty: 2,000 Academic: 5,500 Classified:
5,000)
Campus (acres):
Main: 1,000 (400 ha) Arboretum 1,300 (530 ha)
Experimental Research: 6,000 (2500 ha)
Academic programs: Majors: 146 Master’s: 169 Doctoral:
125
Courses offered: 4,546 Sections: 13,112
Classroom space: 431,000 sq. ft. (40 000 m2)
Research Laboratory space: 1.6 million sq. ft. (150 000
m2)
% of students owning computers: 65%
General-access computers on campus: 1,100
Budget: $1,250,000,000 (State support: 28% Research: 40%)
US Rankings:
Research & development expenditures: 3rd
Voluntary support: 5th (among public universities: 1st)
Number of doctorates granted: 2nd
back to Contents
B)
Strategic Planning and Continuous Improvement:
B1) The Quality Culture at UW-Madison:
The first impact of quality at UW-Madison is already visible on its
website where the Chancellor David Ward presents the annual report
and the perspectives. For the next decade, UW-Madison has planned an
ambitious management project called “A vision for the
future” which gives the priorities, the objectives of progress
and the strategic planning process [Ward, 1999].
Two diagrams show very clearly the effect of such quality approach on
the management organization at UW-Madison. First, figure 03 shows the
strategic planning used since 1988, which is based on Deming’s
quality principles, ie Plan, Do, Check, Act.
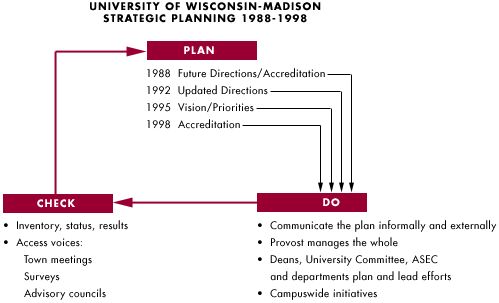
Fig 03: The Deming’s method at UW-Madison
Madison since 1988 up to today
back to Contents
In this strategic planning, the most important is the
“Check” after “Plan” and “Do”, which
involves the obligatory measure of the process results. This Check
process and the involved analysis of the gap between results and
attempts, have a direct effect on the future planned decisions. That
is the reason, it is very important to accurately define indicators
and to rigorously manage the organization in order to obtain them as
precise and credible as possible.
In a such “looped management system”, the University is a
learning and thinking organization which is able to measure its
progress, to understand its gaps and to improve its processes
[Cotter, 1996]. It is expected, and now proved by experience,
that the energy, time and money spent by the organization to provide
all services according to its mission, is better controlled than in
an opened management system where all decisions are only planned and
done without serious and quantified success feedback for the upper
management team.
The second diagram (figure 04) shows how mission can be dispatched in
several priorities after filtering by the vision themes for the
future at the University.
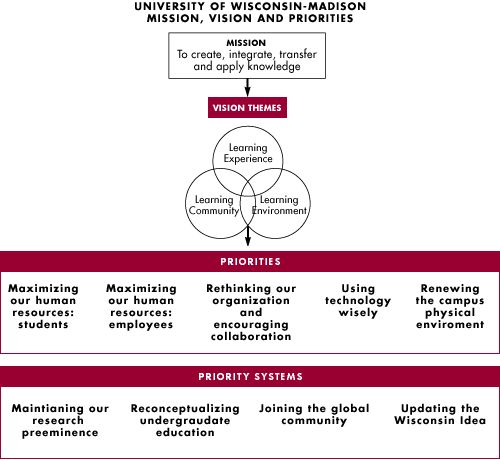
Fig 04: Missions and effects of the “Vision for
the future” project on UW-Madison priorities
back to Contents
B2) Strategic
Planning:
The quality concept used permanently and at all levels at UW-Madison
is the “Strategic Planning Model” (figure 05) [Paris,
1999b]:
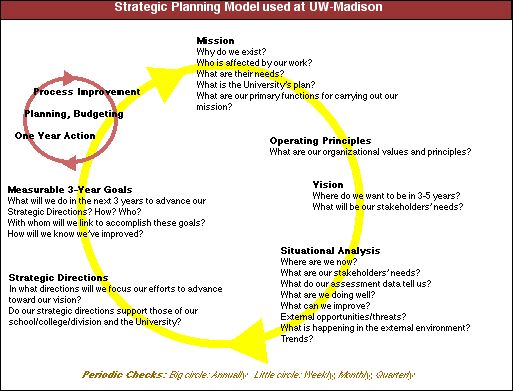
Fig 05: Strategic Planning Model
Strategic planning is a means of establishing major directions for
a department, research team or all other entities at the University.
The aims are to concentrate resources in a limited number of major
directions in order to maximize benefits to stakeholders (students,
employers of graduate, funding agencies, and society, as well as
internal stakeholders such faculty and staff). The methodology is
based on Deming’s philosophy which advises to manage all
processes with a feedback about gap between results and attempts in
order to analyze them and to find solutions to improve processes
[Deming, 1994]
Though strategic planning is a structured approach to anticipating
the future, it is not long-range planning. Strategic planning is much
more sensitive to the external environment than long-range planning
which is traditionally inwardly focused with goals and objectives
taking minimal attention to the larger system in which the
institution functioned. Strategic planning relies on information from
internal and external stakeholders regarding their needs,
expectations and requirements as the foundation for planning. If
traditional long-range planning assumes that the future will be a
linear extension of the present, strategic planning is much more
likely to result in a deliberate shift in direction or refocusing
direction in light of changes, actual or anticipated [Paris,
1999b].
back to Contents
B3) Continuous
Improvement:
The continuous improvement process generally used at UW-Madison is a
seven steps process (figure 06) based on Juran’s and
Deming’s quality management methods [Deming 1989; Juran
1992]
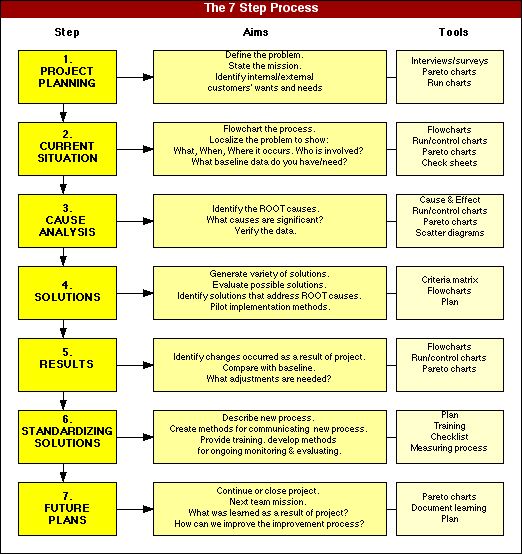
Fig 06: The 7 step process used at
UW-Madison
back to Contents
An “Accelerated Improvement Process” has been
designed by the Office
for Quality Improvement7
at the end of 1999 that enables a team to quickly improve
or create a process (figure 07) [Cotter, 1999].
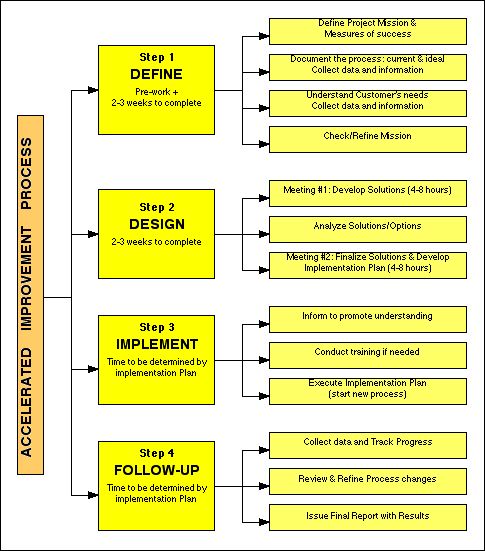
Fig 07: “Accelerated Improvement Process”
designed by OQI at UW-Madison
back to Contents
The requirements of the Accelerated Improvement Process are
leadership commitment and support, the expertise and knowledge of
staff and customers, eventually one facilitator. This accelerated
process is useful for already experimented team in quality management
and continuous improvement. The principle of the Accelerated
Improvement Process is as follows:
- a majority of the project work (data
collection, flowcharting, planning etc...) is done outside formal
meeting time.
- meeting time is spent on generating solutions, prioritizing
solutions and developing implementation and action plans.
- multiple tasks are done simultaneously.
- team meeting time is concentrated into 2 very structured
meetings.
All quality plans developed by research teams, academic departments
or other entities at UW-Madison need measures of success. They are
the criteria that show the impact of the quality improvement, they
can be quantifiable or qualitative, but they must be observable in
some way. Without data on what is being accomplished in the quality
plan, there are little or no foundation for decision making or
improvement. Without data, anyone’s opinion is as good as anyone
else’s. Without knowing in advance what “success”
looks like, it is very difficult to implement any plan. In order to
help everybody concerned by measures of success, a very interesting,
simple and efficient methodology is proposed at UW-Madison
[Paris, 2000].
back to Contents
C)
The operational
organization around Quality at UW-Madison:
There are several organizations, office and center, at UW-Madison in
order to help it to reach its mission, objectives and priorities.
Office
for Quality Improvement
(OQI)8
:
Established in 1994, OQI provides provides consultation
and facilitation services for academic and administrative units
throughout the UW-Madison. Its position at Bascom Hall, closed the
Chancellor’s office, shows clearly the strategic importance
of OQI for the University.
OQI facilitates the use of planning and improvement methods for
any voluntary university teams, helps them to identify their aims
and suggests methods for achieving them. A dozen of members and
consultants9 assist the teams
with all aspects of a quality project like its design, strategic
planning, improving processes, training etc...
They use all well known quality management tools like flowcharts,
cause-effect diagrams, Pareto charts, histograms, check sheets,
control charts and scatter diagrams [Mizuno, 1988].
They already have served numerous university customers like the
following academic departments or services:
|
Academic Advising
campus-wide
|
Academic Services, School &
Education
|
Academic Students Affairs, Grad
School
|
|
Accounting
|
Arboretum
|
Center for Biology
Education
|
|
Chemistry
|
Dean of Students
|
Dean’s Council
|
|
Division of Academic
Services
|
Educational Psychology
|
Engineering
|
|
Entomology
|
Graduate School
|
History
|
|
Housing
|
Integrated Student Information
System
|
Journalism & Mass
Communication
|
|
Mathematics
|
Medical School
|
Pathology & Laboratory
Medicine
|
|
Provost’s Staff
|
Registrar’s Office
|
Research & Sponsored
Programs
|
|
Student’s Academic Affairs,
L&S
|
Wisconsin Food System
Partnership
|
Zoology
|
back to Contents
The quality projects currently in development are:
- Expediting Grant Proposals: A Guide
for Improving the Grant Proposal Process with Examples from the
Department of Medical Microbiology & Immunology
- Using Quality Function Deployment to Improve Academic
Advising Processes
- How TQM Helped Change an Admissions Process
- Redesigning the Industrial Engineering Curriculum at
UW-Madison for a Changed World
- University Housing Food Service Improvement Project
- Chemistry Department Filing System Improvement Project
(coming soon!)
Of course, OQI uses also for itself total quality management
(TQM) methods and has some operating principles to conduct its
daily business like to listen carefully the clients, achieve their
outcomes, model the best practices of a quality-driven
organization, share ideas, successes and failures, respect
diversity and personalities in the interactions, explore
alternatives and take risk in order to create change and
continuous improvement.
Its web site provides a lot of useful information and tools about
Strategic Planning and Continuous Improvement. Since January 1998,
the
“Exchange” newsletter is online on the
net10 . This
bimonthly newsletter of about 15 pages is edited and distributed
freely in order to circulate the quality “culture”,
methods and tools over the university.
The budget of OQI is entirely provided by UW-Madison in order to
allow the stronger focus on its priority aims to serve as better
as possible Mission and Vision of the University. There is no
financial consideration with university customers and according
OQI Director it is an attractive thing for those interested by
quality but not ready to spend a lot of time and money for that.
OQI staff members provide a lot of training sessions on quality
tools, methods and management. They don’t use any specific
quality management software, only Internet browsers and classical
word processors, e-mail and database software. They publish a lot
of internal guides about quality which are of course freely
distributed and easily accessible for everybody.
The measure of success for OQI is based on the results of the
quality projects of their customers. The ratio of projects with
results on total managed projects as well as feedback and repeats
of customers are good indicators of the OQI processes.
back to Contents
Center
for Quality and Productivity
Improvement
(CQPI)11
It is a research center founded in 1985 by Professor
George E.P. Box and the late Professor William G. Hunter. Its
mission is to conduct innovative practical research on concepts
and methods of quality improvement, to provide a national and
international forum for the exchange of ideas among faculty,
students, experts, and practitioners from industry, government and
academia; and to disseminate research findings and ideas through
effective instructional and communication approaches. Its Director
is François Sainfort who I thank a lot for its invitation
to stay at CQPI in order to study quality experiences at
UW-Madison.
For that CQPI disposes about 300 m2 in the WARF12
building within University Campus, has about 20 faculty
affiliates, 6 staff, 10 graduate students, 10 external members,
and 5 to 6 visiting researchers per year. In order to keep the
best scientific level, any faculty member is permanently affiliate
at CQPI, instead all have a university department where they teach
and research. CQPI is a center where the multi-disciplinary
quality problems are studied, requiring input from and interaction
among many different fields. Thus it regroups different origins of
faculty members interested to work about quality problems. Three
mains sponsors help CQPI: UW-Madison College of Engineering,
Graduate School of Business and the College of Letters and Science
via the Department of Statistics. The industrial and scientific
research comes from big international companies but also from
public resources like the National Science Foundation, the State
of Wisconsin, and the UW-Madison Graduate School. More than 170
reports (part
of them accessible online13
), 250 journal articles, 9 books have been authored, co-authored
and/or issued.
CQPI provides also courses and high-level seminars to train
experimented engineers, managers, statisticians about the last
techniques, methods and mathematical tools used in quality control
or management.
back to Contents
Quality
Assurance Systems Research Consortium (QASRC)14
:
QASRC is a consortium which made business in partnership
with the University of Wisconsin-Madison. It conducts study,
development or applied research on problems and issues related to
implementing quality assurance systems. The studies may be done by
faculty, student teams or independent graduate students. The
consortium holds an annual conference and several seminars or
workshops for engineers and managers.
Madison
Area Quality Improvement
Network
(MAQIN)15
MAQIN supports workplace learning, growth and change for
individuals and over 170 organizations in Wisconsin and
surrounding states. Over 60 programs and learning events a year,
and customized assistance to members are provided to the members.
MAQIN members are diverse including the private and public
sectors, manufacturing and service sectors.
back to Contents
Chapter 2
Quality Teaching & Learning Experiences at
UW-Madison
|
A) UW-Madison
Teachnig Academy16
:
In response to a recommendation by the Committee on Teaching
Quality, Evaluation, and Rewards Committee (1989 and 1992), the
Faculty Senate created the Teaching Academy on December 6, 1993. The
Teaching Academy, composed of faculty members and instructional
staff, provides leadership to strengthen undergraduate, graduate, and
outreach teaching and learning at the University of
Wisconsin&endash;Madison.
The long-term goal of the Teaching Academy is to promote effective
teaching and learning on this campus and also nationally, by
encouraging innovation, experimentation, and dialogue among faculty,
instructional staff, and teachers of the future. Thus, the Teaching
Academy is in charge to encourage Excellence in Teaching and to
maintain and further the diversity of teaching excellence across the
university.
The basic functions of UW-Madison Teaching Academy are the
following:
1. Provide a forum for dialogue on
effective teaching-learning.
2. Clarifying criteria and procedures for assessing the quality
and effectiveness of teaching
3. Communicate the best practices of teaching-learning.
4. Encouraging provision of assistance and resources to enable
interested faculty members and instructional staff to improve
teaching
5. Link individuals interested in improving the teaching-learning
process.
6. Sponsor professional development events.
7. Analyze issues and make recommendations on University policies
affecting teaching-learning.
Providing opportunities for discussion of issues in teaching,
research, scholarship, and learning.
8. Create a learning community for sharing for the future.
The Teaching Academy includes outstanding teachers who represent a
broad range of content, teaching styles, and learner characteristics.
It focuses campus and departmental deliberation on issues that are
central for strengthening teaching and learning.
back to Contents
Like a lot of Departments or Services at UW-Madison, the Teaching
Academy uses also strategic planning for its development and
management (figure 08):
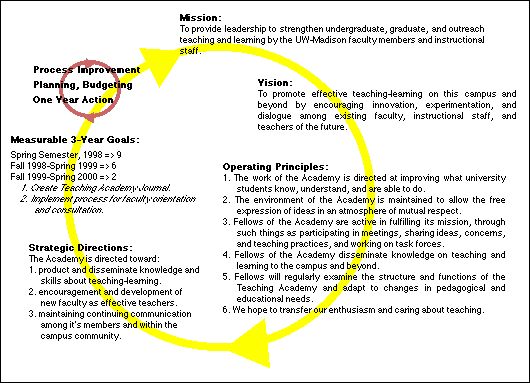
Fig 08: Strategic Planning of the Teaching
Academy
back to Contents
Issues and results:
Yearly, the Teaching Academy identifies and addresses particular
issues to the preceding Committees (Teaching Quality, Evaluation, and
Rewards):
1. What is involved in good teaching?
Dialogue could focus on discussion of the mission of the
university in relation to teaching. Central to this dialogue is an
exploration of what counts as good teaching and how it is
rewarded. Does the current system encourage or discourage a
serious interest by faculty and staff in teaching? Ways to reward
departments that give special attention to teaching improvement
could be explored.
2. How can we develop new partnerships with students so that they
feel actively involved in the educational process instead of being
passive consumers? What changes in curriculum, in the organization
of classes and in pedagogy would lead students to become more
involved? In what ways can we promote active learning by
students?
3. How can we develop criteria for judging excellent resident
instruction and outreach teaching? Teachers often feel
uncomfortable with the way in which they are evaluated by
students. Some students are concerned the evaluation tools used by
teachers are inadequate. Issues of how to measure both teaching
and learning are complex. Other vehicles of evaluation could be
explored?
4. How can we help new and continuing teachers develop their
teaching approaches? What strategies and methods work best in the
classroom? How can we recognize the importance of a diversity of
effective teaching styles and methods? How can we encourage
sharing among teachers to offset isolation and to enrich and
sustain career-long faculty development?
All members of the faculty and instructional academic staff are
eligible to be Fellows in the Teaching Academy for three-year. The
selection of Fellows reflects the scope of campus perspectives and a
variety of teaching approaches.
The work of the Teaching Academy occurs within five Task Forces.
These were created to provide a mechanism that generates
recommendations for constructive change. In addition, the meetings,
interest groups, workshops, seminars, and conferences are designed to
provide opportunities for learning and sharing of what others have
done and what ideas and possibilities are appropriate for this
campus.
back to Contents
The 5 thematic Task Forces are:
Being New and Teacher Preparation
How to support, encourage, and share
teaching experiences with beginning colleagues as well as
graduate students who are considering the teaching profession.
The 1998 report on ”Perspectives
on Being New and Teacher-Scholar
Preparation”17
is available on the web.
Celebrating Effective Teaching
How to communicate good teaching and
provide guides and examples of outstanding university teaching
which could provide benefit.
Instructional Technology
How to rigorously evaluate the impact
of information technology on learning, which could be profound
if it is implemented effectively, supported adequately. In May
1997 this Task Force completed a “white
paper on instructional
technology”18
available on the web.
Peer Review of Teaching
In conjunction with the
American
Association of Higher Education19
, Peer Review of Teaching Project, the Teaching Academy is
monitoring this effort to provide input and encouragement for a
valid experiment on the UW-Madison research campus. Peers are
essential for any valid assessment process and how to do this
efficiently is the challenge ! An action
plan20
is available on the web.
Student Assessment of Learning
In order to examine the available
methods of assessing the students' perceptions of their
learning experience. The validity of student questionnaires,
the content of the questions, the use of the information, and
the evaluation of the results by peers are all being examined
by this task force so that appropriate recommendations can be
generated.
Results of the Task Forces works are very operational, like for
example to provide a “Teaching
Ideas Network”21
for faculty/staff who are searching for assistance with their
teaching. Some Teaching Academy members interested in working with
faculty who are in search of a solution to a teaching problem, are
listed on the web in order to be contacted.
back to Contents
B)
Creating
a Collaborative
Academic Environment (CCAE)22
:
Creating a Collaborative Academic Environment is a movement that
evolved out of Katy Sanders’ Industrial Engineering dissertation
in 1993. Participants in an experimental program found the experience
so rewarding that they asked the Dean to establish the program
college-wide.
At the heart of all programs and projects lies the intent to give
faculty and staff a place to explore non-traditional approaches to
work and collaboration. One of the goals of CCAE is to provide a safe
place and stimulating activities for participants to address complex
issues, consider new directions, create their own solutions and
implement them with supportive from diverses disciplines.
Creating a Collaborative Academic Environment (CCAE) designs and
supports cross-disciplinary professional development programs for
faculty and staff volunteers to work in small groups to explore
theory, question personal assumptions, create new approaches to work,
and nurture each other's growth in teaching, research, and
service.
Several programs designed by CCAE staff, as well as programs
developed in collaboration with other offices on campus contribute to
the campus Vision Priorities of reconceptualizing undergraduate
education, encouraging collaboration, and rethinking the
organization.
Creating
a Collaborative Learning Environment
(CCLE)23
:
The Mission of CCLE is to implement a grass-roots,
faculty advised professional development process that centers
on the construction of knowledge in faculty teams. CCLE
provides a support structure for group work, exposure to
general educational information, and preparation for
practitioner action in the classroom. Volunteers are asked to
make a commitment to attend team meetings, to share their
experiences in teaching and learning, to cooperate with other
participants, to consider new ideas, perspectives, and
techniques, and to eventually be a resource for each other. It
is a unique opportunity to collaborate with colleagues to
explore learning at UW-Madison !
Since 1993, over 130 faculty and instructional staff from 54
departments have participated in CCLE. Each year about 20-25
new participants begin the CCLE program and approximately 20
return to participate in advanced teams. Participants are asked
to make a commitment to:
- focus on developing and expanding
a deep and personal understanding of the learning process as
a precursor to talking about teaching
- attend weekly team meetings (1.5 h/w)
- share experiences in learning and teaching
- be open to engage new ideas, perspectives and
techniques
- be a resource for other faculty over multiple years
back to Contents
Peer
Review of Teaching (PRoT)24
:
Peer review of teaching refers to the participation of
colleagues in the development and/or evaluation of one’s
teaching activities.
1) By colleagues, means
persons who engage in the same or similar kinds of
educational activities, persons who share content expertise,
or persons who bring relevant specialized skills to the task
of peer review.
2) By development, means the creation or evolution of
educational activities over time. Formative review refers to
activities designed to contribute to the development of
teaching. A formative review results in feedback to the
instructor.
3) By evaluation, means the assessment or appraisal
of the quality of someone’s teaching. Summative review
refers to activities designed to produce or provide input to
such an evaluation. A summative review usually results in
documentation that may be reviewed by others.
An other very interesting program still in project is "Creating
a Collaborative Research Environment" which should be organized
like CCLE.
All of these programs are free for participants who have not to
expect any direct professional evolution after they completed them.
The progress, the wanted improvement, is only for the intrinsic
development of each individual, and their motivation must be only to
get better in your job, to be curious to share ideas and experiences
with other people who work in very different areas.
The measure of success and data come from interviews of each
participants and evaluation criteria are only qualitative.
There is no doubt that these methodologies to improve Teaching,
Learning and maybe Research environment at the University will
provide the best way to reach "Excellence".
Some authors and faculty propose to implement Excellence in Higher
Education from the Malcolm Baldrige criteria [Ruben 1997, Steudel
1999]. It is obvious that such plans must be developed from a
strong commitment of all faculty and staff members, that is why the
CCAE approach is promising for the future at the UW-Madison.
back to Contents
Chapter 3
Research & Quality Management
Experiences at UW-Madison
|
A) Continuous Improvement at
Research
& Sponsored Programs25
:
The Office of Research and Sponsored Programs (RSP) promotes and
facilitates research, education, and outreach missions of the
University by supporting and administering extramural sponsored
programs.
The Office of Research and Sponsored Programs (RSP) is responsible
for the final review, negotiation and submission of all grants and
contracts. RSP provides the financial administration of sponsored
research grants and contracts by preparing financial reports,
submitting invoices and processing payments. The primary functions
include the following:
- Transmit extramural support
applications (approx. 3,000 per year)
- Negotiate and accept awards on behalf of
The Board of Regents of the University of Wisconsin System. ($553
million in FY99)
- Administer accounts on a daily basis
(approx. 9000 active accounts)
- Provide training on UW-Madison and
Sponsor's policies/procedures for administrators and
investigators
- Maintain the extramural support
database
- Collect receipts and prepare financial
reports/invoices
- Manage the personnel activity reporting
system (PAR)
- Perform indirect cost studies (Facilities
and Administrative costs)
- Produce a monthly electronic
newsletter
It is integrated into the Graduate School Administration
Organization which contains two Services : Graduate Education and
Admissions Services; and Research Administrative Services where is
RSP.
back to Contents
Since 1997, RSP is performing a continuous improvement on its
processes and the strategic planning methodology is used:
- Mission statement (presented
above)
- Operating principles: Professionalism, Quality
of Service, Office Environment
- Customers: definition of the primary and
secondary customers
- Critical processes:
Proposal Submission:
- Encouraging the pursuit of
extramural funding and identifying funding opportunities
- Proposal preparation
- Regulatory compliance
Grant and Contract Awards:
- Setting-up the Award Account
- Managing the Award
- Trends: list of trends influencing Vision and
Priorities for RSP
- Vision: RSP is the respected leader of
the campus Research Administration Team, fostering
UW-Madison’s continued research preeminence.
- Strategies to achieve the Vision: Build
capabilities and independence, Redesign information technology
infrastructure, Promote professionalism
- Quality action plans (6 months, one-year, more than
one-year)
According to Lois Brako, Assistant Dean at RSP, in charge of this
quality development, it is a good way to clarify the activities of
everybody into the Service but also with customers or stakeholders.
Now, a clear dispatching of roles and responsibilities, between the
Principal Investigator (PI), the Chair of the Service or Department,
the Dean or Designee and RSP, is defined, available, easily
accessible26 and used by every
researcher at UW-Madison.
RSP provides also a lot of training, seminars and helpful information
guides about safety in experimentation27.
back to Contents
B)
Biomedical
Engineering Department (BME)28
:
Biomedical engineering began at the UW-Madison in 1962, and research
topics include such diverse areas as neurological modeling, new
treatments for Alzheimer's disease, biomedical sensors,
cardiovascular system simulation, biomedical instrumentation,
biomedical computing and signal processing, imaging, biomechanics,
rehabilitation engineering and ergonomics, bio-electronic systems and
interfaces...
The Biomedical Engineering Program also received a $1 million grant
from the Whitaker
Foundation29 , under
that organization's Special Opportunity Awards in Biomedical
Engineering program. This has enabled the UW-Madison BME Program to
continue growing, and there are many exciting new developments
anticipated in the next few years as a result of this support.
(A list
of funding agencies30
containing helpful information for
researchers in all fields of science and technology was conceived by
Pr
Gabriel Robins31
. There is also the service provides by RSP at
http://www.rsp.wisc.edu/funding.html).
Quality in this BME research area is achieved by high motivation of
students, strong and efficient team working, high rate level of
international scientific communications, publications and books. The
different security and safety problems which could appear about
experimentation, are well managed by efficient student training in
one of the numerous specific courses available at UW-Madison. The
capitalization of the scientific knowledge is done naturally by the
know-how of the permanent staff like Professors or Assistant
Professors.
BME Department is a recent one at UW-Madison and its Chief contacted
recently the Office of Quality Improvement (OQI) in order to start a
strategic planning approach. This one is only at the beginning but
will allow to the BME research team to focus on priority selected
areas, after having clearly defined Mission and Vision of the
research team. That could be a very efficient way to anticipate the
future and to reach the Excellence in their research area.
The Master of Science degree in BME exists at UW-Madison since 1974.
In recent years, the BME degree program has greatly expanded.
UW-Madison now offers degrees at the undergraduate and graduate
levels (BS, MS & Ph.D. in Biomedical Engineering). The Bachelor
of Science degree began in 1998 with a first promotion of 20
students, the next year the second had about 40.
UW-Madison doesn’t provide a Clinical Engineering program (in 4
years to teach clinical engineers who work in hospital) neither a
Biomedical Engineering Technology diploma (in 2 years to teach
hospital biomedical technicians). In the USA, the 16 Universities
which provide Clinical Engineering programs and the 8 Universities,
Colleges or Institutes which teach BME technology are listed in the
following web list :
back to Contents
US Universities which provide Biomedical Engineering Courses
[accreditation date]:
(source:
http://www.abet.org/accredited_programs/EACWebsite.html)
16 Programs accredited by the Engineering
Accreditation Commission (course level: engineer):
Duke
University, Durham, NC
[1972]
Rensselaer
Polytechnic Institute, Troy, NY
[1972]
Case
Western Reserve University, Cleveland, OH, [1977]
Louisiana
Tech University, Ruston, LA
[1978]
Tulane
University, New Orleans, LA
[1981]
Northwestern
University, Evanston, IL
[1982]
Boston
University, Boston, MA
[1983]
The
Johns Hopkins University, Baltimore, MD
[1983]
Marquette
University, Milwaukee, WI
[1983]
University
of Iowa, Iowa City, IA
[1986]
Wright
State University, Dayton, OH
[1988]
The
Catholic University of America, Washington, DC
[1990]
Vanderbilt
University, Nashville, TN
[1992]
Milwaukee
School of Engineering, Milwaukee, WI
[1990]
University
of Miami, Coral Gables, FL
[1997]
University
of Wisconsin-Madison*, Madison, WI
[1998] (*: not
still officially accredited)
8 Programs accredited by the Technology Accreditation
Commission (course level: technicians):
State
Technical Institute at Memphis, Memphis, TN
[1976]
Pennsylvania
State University, Wilkes-Barre, PA
[1979]
Pennsylvania
State University, New Kensington, PA
[1985]
Cincinnati
State Technical and Community College, Cincinnati, OH
[1988]
State
University of New York at Farmingdale, Farmingdale, NY
[1989]
Owens
Community College, Toledo, OH
[1989]
Gateway
Community-Technical College, New Haven, CT
[1996]
Chattahoochee
Technical Institute, Marietta, GA [1999]
back to Contents
Chapter 4
University Hospital & Quality
Management Experiences at UW-Madison
|
A) About University of Wisconsin Hospital and
Clinics32
:
University
of Wisconsin Hospital and Clinics (UWHC) (figure 09) has
been established by the Wisconsin Legislature in 1924. It has a
fourfold mission: delivery of comprehensive, high-quality patient
care; education of the next generation of health care professionals;
research leading to advances in medical care; and service to
communities throughout the state. In addition of the UW hospital,
there are 12 clinics associated to the UWHC system.

Fig 09:
University of Wisconsin
Hospital and Clinics
back to Contents
For 1999, its budget is about $360 million with the following
statistics : (source:http://www.uwhospital.hosp.wisc.edu/)
- Inpatient Admissions: 21,000
- Outpatient Visits: 460,000
- Emergency Department Visits: 30,000
- Physicians: 700 (active only)
- Number of Employees: 4,000 full-time equivalents
- 474 beds, whose:
- Five intensive care units with a
total of 59 beds
- Trauma and Life Support Center (Level One): 24 beds
- Pediatric ICU: 12 beds
- Cardiac ICU: 8 beds
- Cardiothoracic surgery ICU: 8 beds
- Burn unit: 7 beds
- 20-bed psychiatric unit
- 10-bed security unit
- More than 80 outpatient clinics, including primary
care
The major programs of the UWHC are:
- UW Comprehensive Cancer Center: one of approximately 35
federally designated centers for cancer treatment and
research.
- UW Children’s Hospital: 60-bed pediatric hospital within UW
Hospital and Clinics, nationally known for treatment of
children’s lung diseases and other pediatric specialties.
- Transplant program: one of the nation’s most comprehensive
and successful transplant programs.
1998 Transplants:
- Kidney: 267
- Pancreas: 61
- Heart: 34
- Liver: 73
- Lung: 23
- Small intestine: 1
- Lung/heart and other multiple organ transplants also
performed.
- Ophthalmology: leader in eye research, especially in diabetic
retinopathy, age-related eye disease, ocular melanoma. Ranked
second nationally in federal research support.
- Stroke Center: offers one of the most comprehensive sets of
stroke studies in USA, including testing of multiple surgical
interventions, advanced diagnostic imaging and medications and
therapeutic interventions for acute stroke and its
after-effects.
back to Contents
B)
Quality Improvement Department:
B1) Strategic Planning:
Quality management in UWHC begins by its Mission, Vision and
Goals, which are very explicit:
Mission
Patient Care: To deliver
comprehensive, high-quality health care to patients...
Education: To provide an environment suitable for
instructing medical and other health professions students,
physicians, nurses, pharmacists...
Research: To sponsor and support research in the delivery
of health care and applying the advances in health
knowledge...
Outreach/Community Service: To assist health programs and
personnel throughout the state and region in the delivery of
health care.
Vision
To guide its fulfillment of these
missions, UW Hospital and Clinics has adopted the following vision
statement: To be Wisconsin's foremost health care provider and
employer, serving as a statewide and national leader for patient
care, education, research and community service.
Strategic Goals
1. Strengthened Integration. Align
the vision, goals and operations of the UW Health
organizations.
2. Management of Care. Improve the management of care,
focusing on appropriate utilization of clinical resources.
3. Management of Costs. Maintain a strong and competitive
financial position through stringent control of operating
expenses, prudent capital investment and strengthened fiscal
accountability.
4. Continuum of Care. Strengthen and expand the continuum
of care, emphasizing development of non-acute care services and
tools to manage population health.
5. Network Development. Pursue a multi-faceted network
development strategy encompassing primary care, managed care and
specialty care packages.
6. Clinical Research. Strengthen capabilities in clinical
research through enhanced organization, investigator training and
recruitment.
7. Clinical Education. Adapt educational programs to mirror
and support changes occurring in health care delivery while
promoting new mechanisms for funding this important societal
role.
8. Outreach and Community Service. Strengthen community
visibility and involvement through a more coordinated,
comprehensive outreach and community service program.
9. Communication and Customer Service. Improve
communication and service to all customers of UW Health-including
patients, referring physicians, employers, insurers, fellow
employees and the public at large.
back to Contents
B2) Plan for Organizational Performance
Improvement:
(source: UW Health, Plan Org. Perf. Imp., Internal
Doc., UWHC, june 1999, pp 1-16, r10.05).
In order to serve its strategic goals, mission and vision, the
UWHC uses a Plan for Organizational Performance
Improvement.
The purpose of such quality plan is to assure that health care
services delivered to patients are appropriate, efficient, effective,
safe, and consistent with professionally recognized standards of care
and that the efforts to improve performance are ongoing and
integrated throughout the organization. Due to the rapidly changing
nature of health care, the plan incorporates Continuous Quality
Improvement, Clinical Evaluation and Outcomes Research activities.
The organization should be characterized principally by patient
focused, provider oriented, no boundary between ‘quality’
and ‘management’ of care, accountability for quality of
care, patient satisfaction and resource utilization.
Performance improvement is achieved through the establishment in each
department or service by the implementation of a relevant agenda of
ongoing performance measures, case reviews, and process improvement
projects. Performance improvement is ultimately tied to the
fulfillment of the Hospital’s Mission and achievement of its
Vision.
Beyond the voluntary hospital accreditation, the quality management
method used at UW Health is the continuous improvement of the
processes by which services are provided to meet, and exceed the
needs and expectations of patients and their families, students,
employees and member of the community.
This method is based upon several principles of quality:
- Commitment and involvement on the part
of leadership, including the Board, Medical Staff, Administration
and Department Managers.
- Most problems and opportunities for improvement are tied to
process weaknesses, not to individuals. Therefore, performance is
best improved by focusing on systems and processes rather than on
individuals.
- Performance improvement must be focused on the patient and
coordinated across disciplines and departments. It depends also on
information and data which need to be used to confirm the
existence of problems, identify opportunities of improvement and
evaluate the effectiveness of process improvement. Decisions
should be made based on data, not on intuition alone.
- Employees who are directly involved with a process are best
qualified to improve it.
- Performance improvement recognizes the need to work in
partnership with other components of the care system to assure
quality.
- Staff are trained and are competent to serve specific
population.
back to Contents
B3) Performance Improvement implementation:
Several elements are needed for success in Performance Improvement at
UW Hospital, like displayed in the cause-effect diagram below (figure
10):
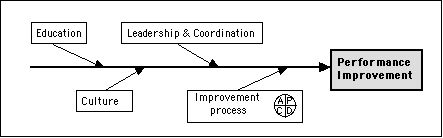
Fig 10: Cause-Effect Diagram of the Performance Improvement Process
at UWHC
Culture: The culture of UW Health is one of
value and trust for employees, medical staff and students focused
care.
Education: all employees, staff and managers need to
learn new skills and approaches for stabilizing and improving
processes. The Director of Clinical Affairs assures the
availability of means by which all hospital members have access to
learning about Performance Improvement methods and tools. The
Hospital also provides a curriculum of continuing education in
quality. Today, the quality trained hospital members are about 400
(10% of the total), and it is considered like well according the
means in teaching staff (only 1 person). Very often, a part of
trained employees are able to train or to explain quality
concepts, methods and tools to their colleagues. This kind of
person becomes a natural leader for a team of about 5 to 10
people. Thus, there is a natural amplification of the training
given by the teaching staff.
back to Contents
The one day quality courses provide by the Clinical
Affairs Department are listed in the figure 11:
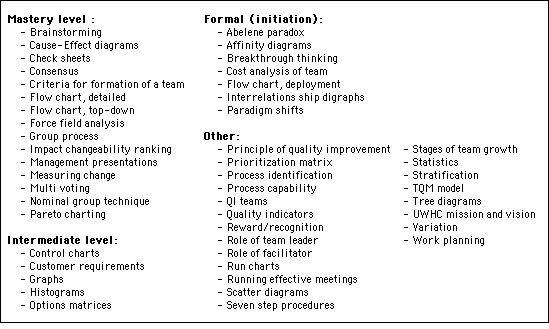
Fig 11: Quality courses at UW Hospital
back to Contents
Very often, there is a little homework for each course.
The role definitions of each actor in the quality team process are
the following:
Facilitator:
Characteristics
- Outside the process and/or the department
- Skilled in data-based problem solving
- Knowledgeable about group process
- Skilled communicator
Responsibilities
- Communicator: keeps all areas informed of quality
improvement activities
- Champion: helps maintain quality improvement progress and
team momentum
- Instructor: instructs in quality improvement process and
techniques
Team leader:
Characteristics
- Supervisor or manager in project area
- Expertise in process
- Knowledgeable about process
- Able to leave rank outside meeting room
Responsibilities
- Designs action plan, agendas and team meetings
- Teaches and leads team through process improvement steps
- Help maintain team momentum
- Communicates and coordinates with all affected and involved
areas
- Meets regularly with management
Team member:
Characteristics
- Knowledgeable about process
- Desire to be involved
- Willingness to speak up
- Ability to commit time and energy
Responsibilities
- Attend and participate in all meetings
- Gather data
- Analyze root causes
- Participate in presentations
- Recommend solutions
- Track effectiveness of solutions
- Establish on-going monitoring (quality control)
back to Contents
Leadership and Coordination: the
organizational structure of the coordination of performance
improvement at UW Health is shown in the figure 12 below, which
illustrates the linkages between the various entities associated
with improving organizational performance:
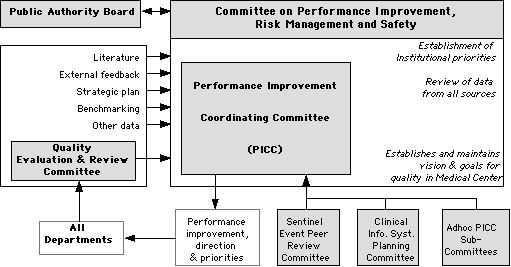
Fig 12: Quality Committees at UWHC
back to Contents
Committee on Performance Improvement, Risk Management
and Safety: the Chairperson of the UWHC appoints 2 Board
members as liaison with this Committee which receives and reviews
detailed performance improvement, risk management and safety
reports. If there is an issue that requires Board action, the
liaisons present the issue to the Board, otherwise, they report to
Board only the broad outlines of activities to assure to the Board
that the process is functioning as approved.
Performance Improvement Coordinating Committee (PICC): It
establishes and maintains the vision and goals for quality in the
Medical Center; integrates about 20 members like medical staff,
nursing, other healthcare providers, hospital administration and
members of quality improvement department and clinical
affairs.
Quality Evaluation & Review Committee (QERC): It is
responsible for oversight of departmental performance assessment
and improvement activities which are accomplished by annual
departmental committee reporting to QERC. QERC is also responsible
for measurement and ensuring compliance with the Joint Commission
on Accreditation of Healthcare Organizations (JCAHO)33
standards. The JCAHO accredits health organizations every 3 years.
QERC includes about 30 members from each medical department which
has its own quality review sub-committee with a meeting every
week.
back to Contents
B4) Improvement process and Quality Improvement
Department:
The Quality Improvement Department supports all quality committees in
hospital, plans and manages quality actions and training, looks after
the quality indicators and reports all interesting information to the
Physician in Chief. It also prepares the renewing of the hospital
accreditation and develops the concrete quality actions following the
Institutional priorities and strategies. UW Health uses approaches
for improvement which include:
- Individual traditional quality assessment activities
and peer review
- Structured method based on the seven step process
- Quality control
The Plan - Do - Check - Act process may entail seven
steps:
Plan:
Step 1: Identify and analyze the
critical process, estimate the gap in quality
- Identify the process
- Flowchart the process
- Identify the customer
- Identify the gap in quality
- Identify team members
- Train team members
Step 2: Master the data, using it,
develop a thorough understanding of the process, establish
specific quality indicator
- Macro-process flowchart
- Validate customer requirements
- Establish quality indicators
- Complete data stratification
Step 3: Probe for the root causes,
analyze factors contributing to problems in the process, search
for, identify and verify actionable root causes
- Determine root causes
- Verify root causes
Do:
Step 4: Review and develop
solutions which address the verified root causes of the gap of
quality, determine that the solutions are cost effective and that
they meet customer requirements. Develop an action plan.
- Select solutions addressing root causes
- Verify cost-effectiveness of solutions
- Verify that solutions meet customer needs
- Develop an action plan
Check:
Step 5: Observe the change.
Solutions are implemented, as pilots if possible, and the results
of the change are measured. Data should demonstrate a closing of
quality gap and elimination of root causes.
- Data demonstrates improvement
- Root causes reduced or eliminated
- Contributes to hospital goals
Act:
Step 6: Verify fit in the
workplace. Successful solutions are identified for
standardization, key indicators and methods are developed and
automation of ongoing monitors is investigated
- Successful solutions identified for standardization
- Standard processes/procedures developed and tested
- Key indicators developed
- Automation of ongoing monitors investigated
- Action plan for continuous monitoring developed
- Plan implemented and communicated
Step 7: Ensure the future, generalize improvements to other
areas, investigate future improvements, share findings, celebrate
achievements
- Explore generalization to other areas
- Additional improvements investigated
- Findings shared
back to Contents
The performance measurement is often the most difficult to do
because the nature itself of the direct or indirect indicators. The
following criteria help to ensure that the data collected are
appropriate for monitoring performance :
- the measure can identify the events it
was intended to identify
- the measure has a documented numerator and a description of the
population to which the measure is applicable
- the measure has defined data elements and allowable values
- the measure can detect changes in performance over time
- the measure allows for comparison over time within the hospital,
or between it and the other health entities
- the data intended for collection are available
- results can be reported in a way that is useful to the hospital
and other interested stakeholders
According the Directors of Quality Improvement Department and
Clinical Affairs, the three success keys of performance improvement
in an organization are:
- Strong, permanent and efficient training of all
hospital members, at all levels
- True and strong commitment and involvement at the top management
staff
- Audacity, still audacity and always audacity for the quality
managers, teams and members involved by continuous
improvement.
back to Contents
C)
Medical
Physics Department34:
The word Medical Physicists groups together physicists who work on
radiotherapy, X Ray radiodiagnostic, US diagnostic and Magnetic
Resonance Imaging (which is a little bit shared with biomedical
engineers) In the USA, medical physicists are about 3000, in
Wisconsin about 70 and in the University Hospital of Madison, they
are about 12.
The Radiotherapy Service uses some specific medical apparatus
like 1 CT Scanner (Siemens), 4 Linear Accelerators (Varian), 1
simulator (Varian) 1 ultrasound unit (Siemens). They also make
considerable use of the imaging modalities in the Radiology
Department. There are 11 therapists and among them 4 are trained to
do daily assurance quality procedures on linear accelerator and
simulator. Four are also trained to perform the quality assurance on
the CT unit.
- daily: 20 mn to check general
parameters on a unit,
- weekly: 90 mn for a more thorough check by the physics staff,
that rotates through a different set of checks over a month.
A Radiation Protection Code has been established by the State of
Wisconsin and is used to plan and manage the minimum about safety and
quality procedures (Wisconsin Administrative Code, Rules of State
Board of Health, Radiation Protection Code, Chapter H 57, January
1966). For Curietherapy and Cobaltotherapy, there are also laws which
impose the responsibility for an institution to do minimal quality
and safety procedures (www.nrc.gov,
Title 10, Part 35). For Linear Accelerators, some new technical rules
are coming soon from the State of Wisconsin.
The Quality Management take several forms in the Radiotherapy Service
of Medical Physics Department. The major quality checks of units and
medical procedures are:
2 times per year:
- Control of measure and test instrumentation ( Thermoluminescent
Light Detection...) used to control patient radiation.
Each year:
- Inspection by the University Safety Department to measure and
control the radiation dose inside and outside the service for
workers, employees and patients.
- Inspection by the Nuclear Regulatory Inspection (Federal
Organization) on the good professional practices and procedures
used by the Department.
Each 3 years:
- Visit by the Quality Review Committee of the Hospital in order
to be ready for the renewing of the Accreditation for all the
Hospital. The Join
Commission on Accreditation on Healthcare Organizations
(http://www.jcaho.org) comes every
three years. The Quality Review Committee of the department meets
every week, and has a representative in the hospital Quality
Evaluation & Review Committee.
back to Contents
In the Radiological Physics Services, the quality
management is permanent, both on the technical control of the X ray
devices (about 80), and on the organization improvement where TQM is
employed.
There are 2 quality committees for the Radiological Services:
- Quality Assurance Committee which
focuses about technical quality of devices in order to do the best
diagnostic
- Quality Improvement Committee which is focused on the ability of
the organization to satisfy the patient and to improve the quality
process.
For the first preceding point, 2 standards give the minimal
rules to be observed:
- Code of Federal Regulations (1994): X
ray => Chapter 21 CFR part 1020
- Wisconsin Administration Code (1982): Radiation Protection Code
HSS 157
The X ray Quality Assurance Manager has an office into the
Radiodiagnostic Service and is permanently helped by 2 medical
physics students to plan, do and check the different procedures
associated to the technical control of the X ray devices. Some
imaging phantoms have been developed by the QA manager himself who
also uses classical testing instrumentation. It is kept track of all
quality records, but at the moment there is still no publication
about the profitability of the quality check by internal service in X
ray upon the quality of the medical diagnostic. It seems obvious that
it is necessary and efficient, but some quantitative proofs could be
very useful for other radiological services which plan to develop
such approach.
back to Contents
D) Clinical
Engineering Department:
The Clinical Engineering Department at the University of Wisconsin
Hospitals & Clinics (UWHC) has one Clinical Engineer has 7
biomedical technicians. It is integrated into the Plant Engineering
Department which is composed of 80 people (figure 13).
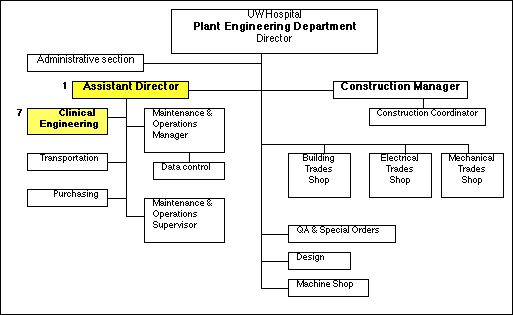
Fig 13: UW Hospital Plant Engineering Department Organization
Chart
back to Contents
The only one Clinical Engineer who is at the head of the CE
Department is helped by another one from the University
Healthcare Consortium (UHC)35
by contract with UWHC. This kind of partnership is often used in US
hospitals in order to compensate the lack of people.
The shops where work biomedical technicians are very small and it is
obvious they need more place to correctly perform their job.
The CE Department has been accredited by JCAHO in fall 1999. A
helpful guide36 is edited by
JCAHO
in order to prepare the accreditation where the chapter 8 is specific
to the Medical Equipment Management.
About requirements and recommendations used daily by the Clinical
Engineering Department, most of them come from AAMI37
, the biggest biomedical professional association in the USA. AAMI
provides professional recommendations or requirements very useful for
clinical engineers and biomedical technicians.
Other sources which provide official, national or international,
standards in clinical engineering are :
- American
National Standards Institute (ANSI)38,
equivalent to the French AFNOR39
- National
Fire Protection Association (NFPA)40
which provides codes and standards about health care facilities,
electrical equipment maintenance and electrical safety.
According to the Director of the clinical engineering department, the
daily use of such codes and standards from these organizations
improves the facility to be accredited.
The ISO 9000 Certification is not an objective neither a priority in
the US clinical engineering departments. Only few of them are
certified, even if the advantages to have a more rigorous
organization and an efficient documentary system are recognized.
back to Contents
Chapter 5
Synthesis and transfer possibility to
the French context
|
My professionnal project is about implementing quality management
methods into public organizations like University, Research
Laboratory and Hospital.
All I have seen during my stay at UW-Madison is available to
implement in the French context and especially Strategic Planning and
Continuous Improvement which are soft and smooth methodologies to
promote quality culture.
Quality is a challenge, and not a battle ! That is why it is better
to begin with voluntary teams into public organization, the essential
thing being to give at each people the wish to develop quality
approach, methods and tools in their daily work, because they will
know working environment will be more comfortable and problems easier
to resolve without psychological strain or bad feelings.
This chapter presents the impacts of Strategic Planning and
Continuous Improvement on proposals to design and manage the two
objectives of my professional project : Quality in Research and
Quality in Hospitals.
back to Contents
A) Quality in Research at UTC:
The project « Quality in Research at UTC » is very
important because it will be the first time, that quality management
principles will be applied at Compiègne University. The
challenge will be to succeed with this first experience in order to
create a good feeling about quality.
According to the Director of the Research Department, quality
management methods and especially continuous improvement will be
tested with a voluntary scientific team41
.
According to the strategic planning model, Mission, Vision and
Priority for the Research Department can be given like possible
examples (figure 14). Of course, these proposals still need to be
discussed and validated, but a good, reasonable and motivating
priority could be to reach the Excellence in Research.
To reach the Excellence in Research, it is necessary to have
excellent researchers with excellent organization. The project
focuses about this second point which can be very often widely
improved. That is the reason, one of the strategic directions is to
implement Quality Management methods and tools in research
organization.
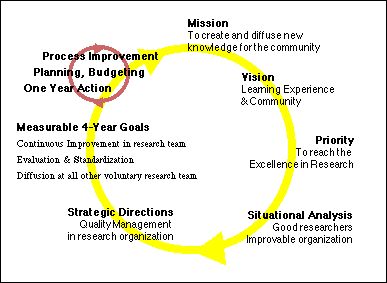
Fig 14: Example of the Strategic Planning applied to
the Research Department at UTC
back to Contents
This involves three measurable four-year goals between 2000 and
2004:
- The first one is to test the real benefits of
continuous improvement with a voluntary research team.
- After that, to evaluate the results of the improvement process,
to understand the gap between them and the attempts, to improve
the processes and to standardize solutions which are really
benefit and progress for the research team.
- The third goal is to communicate about clear, real and proved
gains and advantages in order to lead other scientific teams to
test and use quality management tools and then diffuse quality
into research organization. This way will be not very easy to
manage, that is the reason, it is necessary to choose very
carefully the success criteria for this first quality experience
and not to be too ambitious in a first time.
Concerning the voluntary scientific team, its research is in
majority applied with a lot of industrial contracts and funding. So,
they develop new processes for the environment, agronomic, industrial
food and powder technology areas.
They have numerous technical experimentation sites, inside and
outside the University. That is why, they need to better control
the safety of the experiments (figure 15).
To help researchers, they also use a lot of engineering students who
work to improve for example a part of the experiments. That is
why, they would like to better manage the important turn-over in
order to be secure and efficient with new students.
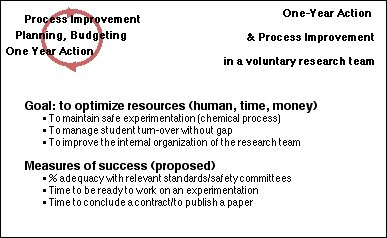
Fig 15: Quality action plan for the voluntary
research team
back to Contents
The team has about 30 permanent researchers and 15 scientific
engineers or technicians. The organization is classic with several
thematic groups, an administrative staff, a scientific council and a
leader. This team is also recognized by the French National Council
of Scientific Research, that means the quality level of its research
is well recognized and approved.
In order to keep the funding level and improve it, in majority from
private and international companies, the team leader would like to
use the same quality culture to give them confidence in his
capacity to understand, to define and to find effective solutions to
their industrial problems. Very often these companies use total
quality management principles, can be also ISO 900042
certified or have some accredited EN 4500043
laboratories like sub-contractors.
But it is no question to spent a lot of time or money for a quality
development, especially when there is no proof it will be really
profitable. That is the reason it will be applied an evolutionary
process and not a revolutionary one.
The general methodology I will propose to use is the 7 step
process of problem resolution which provides a continuous improvement
(figure 16). According to the Director of the Office of Quality
Improvement at UW-Madison, it is really the more efficient way to
begin and control a quality development, because it focuses directly
on real problems and also their operational solutions. This approach
provides the guarantee to optimally spend time, energy and money.
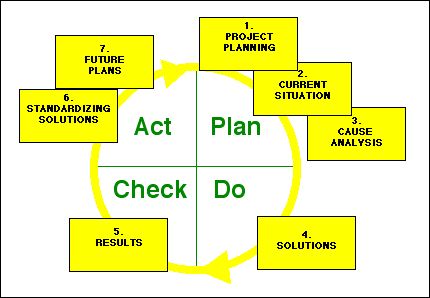
Fig 16: Seven step process of problem resolution
providing continuous improvement
back to Contents
Certainly, some members of the research team could have some
natural reluctance about the change and it is also necessary to be
very careful not to spend too much time in meetings.
For that I propose to apply the advice given by Kathleen Paris from
OQI: fewer meetings but more accomplished !..[Paris,
1999a]. The method is simple:
- first to define a clear understanding
of purpose and also outcomes which are attempted,
- second to decide whether a meeting is really required (there is
not always evidence or necessity for that)
- third to find the best person to conduct the meeting (it is not
necessary always the chief especially when he is strongly
concerned),
- fourth to define and timetable the quickest agenda with the aim
of the meeting at the top and the use of verbs in items to avoid
vague proposals and fuzzy actions,
- fifth to end the meeting with a project timeline where it is
written what it should be done, by whom and when.
In order to be able to reach the two other goals concerning the
Strategic Planning for the Research Department (to evaluate results
and standardize solutions ; to diffuse quality principles at all
other voluntary research team), I suggest to plan to be able to
improve the process of the improvement process implemented in the
research team.
For that, the use of the PDCA cycle is the best way to be credible,
to know what it will be really asked to do, to improve the process
and to be able to widely diffuse the method after this first
experience (figure 17). When it will be necessary to check the
results of the improvement process, a possible and useful indicator
could be the percentage of resolved problems versus the attempts and
the time needed for that [Paris, 2000]
back to Contents
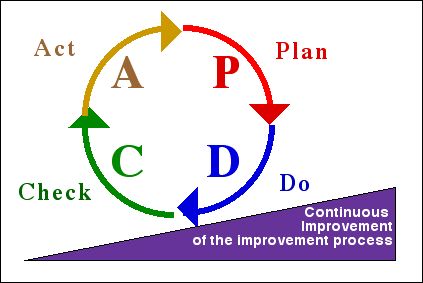
Fig 17: Continuous Improvement of the Improvement
Process
The first step of the project "Quality in Research" is planned on
two years from 2000 up to 2002. After that and if the results are
real, proved, profitable and enjoyed versus the energy, time and
money spent for that, then the Research Department will develop a
« Quality Resource Center » in order to:
- capitalize the first progress in
quality management,
- diffuse the methodology at all other voluntary university
teams and maybe,
- develop some original concepts, methods and tools
especially adapted to the scientific research and higher
engineering education. For example, OQI at UW-Madison has created
an « Accelerated Improvement Process » from its own
experience, which permits to divide by 2 to 5 the time needed to
resolve a problem and implement new solutions [Cotter,
1999]. It is a concentrated version of the 7 step process seen
before.
back to Contents
B)
Quality in Hospitals:
The second objective of my professional project is about "Quality
in Hospitals". If the strategic planning model is applied on this
field, global Mission, Vision and Priority available for all French
hospitals can be defined (figure 18). The last point, the
priority to obtain the French accreditation comes from the new French
law44 which imposes all French
hospitals, public and private, to be accredited before March
2001.
Because Compiègne University teaches Clinical and Biomedical
Engineering since its creation, and has now taught more than 80% of
the French hospital clinical engineers, there is a particular
attention from its managers, especially those in continuing
education, to respond to this new hospital market demand.
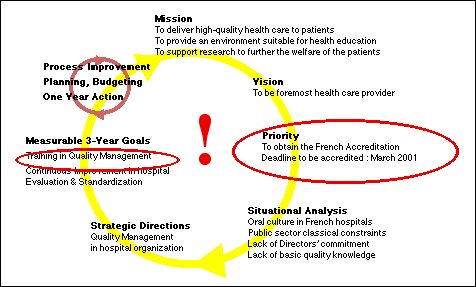
Fig 18: Example of Strategic Planning applied to
French Hospitals
back to Contents
The French hospital accreditation is obligatory, on the contrary
US and Canadian accreditation are voluntary. But both are at the
origin of the French referential, that is why it contains a lot of
total quality management philosophy. In France, Hospital
Accreditation is a subject with an extreme political sensitivity.
Indeed, the President of the Public Hospital Board is the mayor of
the town and the hospital is very often the first or the second
employer of the area. So, it is politically strategic to have a good
hospital, and all problems like strikes or closing of medical service
are not welcome ! That is the reason, accreditation for public
hospital is a political deal, and for private hospital it could be
the only way to survive ! This explains why, all hospitals in France
are rushing to obtain accreditation before the deadline.
Like in all old and public organizations, problems to implement
quality management in hospitals are numerous:
First the old oral culture is shocked by the need to write and trace
all processes with the quality management methods. There is already a
feeling of lack of confidence about the managers who want to
implement such methods and already the beginning of a social strain.
This problem of quality in public sector is the research area of some
researchers at CQPI, UW-Madison, and it could be interesting to
exchange data and experiences in the future.
Second, about the lack of Directors’ commitment, we are helped
in France by the Health Authorities and all upper managers, directors
and CEOs have to take into account the requirements of the
accreditation. This one contains strong inducements to
self-evaluation and quality management at all levels in the
organization. Because there is a lack of quality knowledge and
operational know-how, the Directors’ staff must be urgently
educated. It is now a one-year action for numerous hospitals, and
certainly still for several years !.. At the moment, quality training
in hospital is done by consultants and there is no, or very few,
specific quality courses for healthcare managers. Some Directors or
managers who are in charge of the accreditation, attend and try to
complete efficient quality course in Universities or in Higher
Education Colleges, unfortunately very often focused on industrial
field.
That is why the project "Quality Course" is focused especially on
hospitals in order to train efficiently their quality managers and
all other employees strongly concerned by quality.
back to Contents
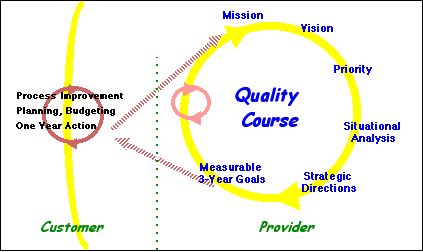
Fig 19: Strategic Planning applied to the Quality
Course Project
Like shown in figure 19, the project replies to a demand which
comes from the strategic planning of hospitals. But it is also
possible to use the strategic planning model for the project itself !
It is interesting to see the effect « Russian Doll » of
this methodology. In fact, each action, each activity could be
managed by a strategic planning. Moreover, with this model, we can
observe the linkage between the potential customer’s needs and
the educational service provided. The inputs of the project Mission
are the customer’s needs. One of the outputs (measurable 3-year
goals) should be obligatory the satisfaction of these customer’s
needs.
For the educational project, the Mission is to train
intensively hospital CEOs, Directors and Quality Managers about:
Concepts of Quality in Healthcare, Methods and Tools of Quality
Management and Specificity of Hospital Accreditation.
To balance the budget, the course should be attractive enough in
order to have each year at least 20 to 25 students. So, the
Vision "to be the most attractive" involves two
priorities:
- First to be efficient, modern and
credible because a lot of very professional consultants are on
the market,
- Second to develop an educational network, a partnership
with other universities or schools because Compiègne
University is specialized in engineering and doesn’t have all
resources for such educational program.
back to Contents
To be efficient, modern and credible, it could be very helpful to
use the continuous improvement methodology. That means to use
the PDCA cycle at each step of the program, Design, Marketing
and so on, but also on the entire educational program itself (figure
20).
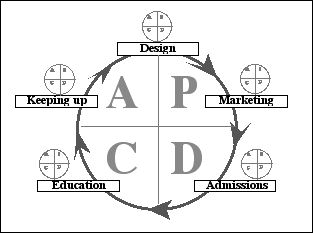
Fig 20: Continuous Improvement applied to the
Quality Course process
The management of such process will be a good way to be
credible because the managers themselves will know what they
will teach and efficient because they could control the entire
process of the educational program and it will be easier to improve
it and to be ready at all market change.
For that it is necessary to design and express clearly and accurately
what it should be done in each step of the process and, maybe more
difficult, what are the inputs and outputs of each sub-process. I
have prepared a very detailed proposal about this management process
which will be discussed between June and August 2000 and maybe
approved by all partners.
back to Contents
At the moment, three partners are in the educational network, each
being complementary of the others:
ENSP is the only French National Public Health
Higher Education School which teaches all public hospital
directors in France. This school depends on Health Ministry and
has a very great impact on new and former hospital managers.
Montreal University because it is a French speaking area
and the origin of the French accreditation comes in part from the
Canadian model. There is also a great experience and expertise
about quality in healthcare.
UTC, because its long teaching experience in Quality for
industry and Clinical Engineering and also there is a long
know-how on distance learning methodology.
The course is designed to be recognized by both Canadian and French
Educational Authorities in order to be useful for the professional
evolution of the applicants. The majority of applicants will be
professional hospital managers certainly in charge of great
responsibilities, most of them could be French and it is planned to
have 20% of Canadian or foreigner applicants. The course will be
provided for a third part like a classic training in each of the
three partners, and the other two third part by distance
learning.
back to Contents
In conclusion, Strategic Planning and Continuous Improvement are
very attractive methodologies and could certainly optimize
dramatically daily work of everybody.
Very often people have to do a lot of things, to make a lot of
decisions without the comprehension of the origins of the problem, or
the impact of their own actions on the others into the organization.
They have no time, they are so busy and they work 12 hours a day. It
is obviously a wrong way, because it is impossible to continue to
control a more and more complex system or organization like that. And
this fact is increasing each day !
A good manager has to do the efficient things at the good moment at
the right place with the right people. For that, it is necessary to
know exactly where, when and how to focus, according to the
organization, department or service : Strategic Planning is really
helpful for that ! People have also to daily minimize the gap between
their results and the attempts of their processes: Continuous
Improvement is the right tool for that ! Both could create a more
comfortable working environment.
I saw at Madison, the real effects of total quality management
philosophy on big organizations in the same field than those I work
in France: University and Hospitals. I really think it is possible to
implement such methods, because there is nothing
“extraterrestrial” but on the contrary a lot of useful and
efficient kind of tools and methods to resolve problems, to find
pragmatic solutions and to be sure they are always working in the
future.
The most important success key is the commitment of the upper
managers, and for that I hope to be convincing, pragmatic and
charimastic enough in order to give them confidence about the
strategy and the attempted results.
I don’t know if the quality of life at Madison comes from the
quality culture of people, or the inverse, but the quality of my stay
in the Wisconsin, and particularly at the University has created on
me a very good feeling to continue my efforts to develop and promote
quality management, simply and efficiently. “Constancy of the
Purpose !” Deming said...
back to Contents
Akao Y & ad., 1991, Hoshin
Kanri: Policy Deployment for Successful TOM, Productivity Press,
Cambridge MA.
Argyris C, 1998, Empowerment: the Emperor's now clothes,
Harvard Business Review, Boston, May/June, Vol. 76, Issue 3, pp
98-105, ISSN 00178012
Asfour S., Iakovou E., Cortes G. A., A Synthesis of Quality
Function Deployment and Robust Design and its Application in the
Medical Device Industry, Quality Engineering, Ed Marcel Dekker
Inc, 1999, 12(1), 37-45
Bechtell ML,1995, "The Management Compass. Steering the
Corporation Using Hoshin Planning, American Management
Association, New York NY.
Bossert J. L., 1991, Quality Function Deployment: A
Practitioner's Approach, ASOC Quality Press, Milwaukee Wl.
Brassard M., 1989, The Memory Jogger Plus+, GOAL/QPC,
Methuen MA, http://www.goalqpc.com
Colletti J, 1995, A Field Guide to Focused Planning: Hoshin
Kanri - American Style, The Woodledge Group (+ 1 203 653 5698),
EastGranby, CT, USA.
Cotter M, 1999, Accelerated Improvement: a
“How To” Guide, UW Service for Planning &
Improvement, OQI, V1.3, November
Cotter M, 1996, Systems Thinking in a Knowledge-Creating
Organization, Journal of Innovative Management, Vol. 2, N°1,
Fall, pp15-30
Cowley Michael & Domb Ellen, 1997, "Beyond Strategic
Vision : Effective Corporate Action With Hoshin Planning,
Butterworth- Heinemann.
Dalrymphe J., Edgeman R. L., Finster M., Guerrero-Cusumano
J.L., Hensler D. A., Parr W. C., A White Paper: Quality at the
Crossroads of Organizational Excellence and the Academy, Quality
Engineering, Ed Marcel Dekker Inc, 1999, 12(1), 97-104
Deming WE,1989, Out of the Crisis, Ed.
Massachusetts Institute of Technology, Center for Advanced
Engineering Study, Seventh Printing, April, p 507, ISBN
0-911379-01-0
Deming WE, 1994, The new economics, for Industry,
Government, Education, Ed. Massachusetts Institute of Technology,
Center for Advanced Engineering Study, Second Edition
Eureka W. E. and N. E. Ryan, 1990, The Process-Driven
Business: Managerial Perspectives on P.O.-cy Management, ASI
Press, DearbomMl
Hermel P., Edgeman R. L., Dahlgaard J.J., History and
Specifics of the Quality Movement in France, Quality Engineering,
Ed Marcel Dekker Inc, 1999, 11(4), 619-624
Hild C., Sanders D., Ross B., The Thought Map, Quality
Engineering, Ed Marcel Dekker Inc, 1999, 12(1), 21-27
Hoonakker P, MacEniry M, Carayon P, Korunda C
& Sainfort F, 2000, Total Quality Management and Teamwork
In the Public Sector: the Wisconsin Department of Revenue Study,
CON, UW-Madison, to be published in June 2000
Gitlow H. S., 1990, Planning for Quality, Productivity, and
Competitive Position, Dow Jones- Irwin, Homewood IL.
JCAHO, 1998, The Environment of Care® Handbook, Ed
JCAHO, 129 pages, ISBN: 0-86688-589-7
Juran JM, 1992, Juran on Planning for Quality, The Free
Press, Collier Macmillan Publishers, London, ISBN
0-02-916683-7
Juran JM, 1988, Juran on Quality by Design, The Free Press,
Collier Macmillan Publishers, London, ISBN 0-02-916681-0
King B., 1989, Hoshin Planning: The Development Approach,
G0AL/QPC, Methuen MA, http://www.goalqpc.com
Masaaki Imai, 1986, Kaizen, the key to Japan's competitive
success, Ed. McGraw-Hill, ISBN 0-07- 554332-X
Masaaki Imai. Gemba KAIZEN, L'art de manager avec bon sens,
Les Editions JV & DS, 33, rue de Vaugirard, 75006
Paris-France, Tel: +33 1 42 84 03 16, Fax: +33 1 42 84 03 31
Masaaki Imai, Gemba KAIZEN, A Common Sense Low-Cost
approach to Management, Publisher: McGraw-Hill, 11 treat New York,
NY 10011, USA, Tel: + 1 212 337 5047, Fax: + 1 212 337 5999, You
may buy it on-line through Amazon book store
Mizuno Shigeru, 1988, Management for Quality Improvement,
The 7 new QC tools, Ed Mizuno Shigeru, Productivity Press, ISBN
0-915299-29-1
Nayalani, Y., T. Eiga, R. Futami, and H. Miyagawa, 1994,
The Seven New QC Tools: Practical Applications for Managers,
Ed Quality Resources, White Plains NY.
Paris K A, 2000, Creating Measures of Success for Your
Plan, UW Office of Quality Improvement, June,
oqi@mail.bascom.wisc.edu
Paris K.A,1999a Fewer Meetings but More Accomplished,
Services for Planning & Improvement, Office of Quality
Improvement, UW-Madison, oqi@mail.bascom.wisc.edu
Paris K A, 1999b,Strategic Planning in the University, UW
Office of Quality Improvement, http://www.wisc.edu/improve,
oqi@mail.bascom.wisc.edu
Ruben BD & Lehr L, 1997, Excellence in Higher
Education, A Guide to Organizational Self-Assessment, Strategic
Planning and Improvement, Rutgers OCI, January, ISBN 0- 7 87 2-45
6 2-3
Sainfort F & Carayon P, 1999, Quality
in the Public Sector: The employees' perspective by Christian
Korunka, Dieter Scharitzer, CQPI, UW-Madison, Report Series in
Quality & Productivity n° 175
Sainfort F & Carayon P, 1997, Total Quality Mangement
in an American Public Sector Organization, 24ème
Congrès International Franco-Québecquois de
Génie Industriel, Ecole des Mines d'Albi
Sheridan B. M., 1993, Policy Deployment: The TOM Approach
to Long Range Planning, ASQC Quality Press, Milwaukee, WI,
USA.
Shewhart WA, 1939, Statistical Method from the viewpoint of
Quality Control, Ed. Deming WE, The Graduate School, The
Department of Agriculture, Washington
Shewhart WA, 1980, Economic Control of Quality of
Manufactured Product, D. Van Nostrand Company Inc (1931),
republished in 1980 by Ed. ASQC
Smith GF, 1998, Quality Problem Solving, Ed. ASQC Quality
press, Milwaukee-Wisconsin, ISBN 0- 8 7 389-394-8
Steudel H, 1999, Implementing Total Quality Management and
Malcom Baldridge-Type Assessments in Higher Education, Dept of
Eng. Prof. Dev., College of Engineering, University of
Wisconsin-Madison, internal training session
Sullivan L. P., 1988, "Policy Management through Quality
Function Deployment, Quality Progress, Vol. 21, June, pp.
18-20.
Van de Van AH, Angle HL, Poole SM, 1989, Research on the
management of innovation: the Minnesota studies, Ed. Harper &
Row, New-York, ISBN 0-88730-331-1
Ward David, 1999, A Progress Report on our Priorities: a
Vision for the Future, UW Office of Quality Improvement, January,
oqi@mail.bascom.wisc.edu
back to Contents
Appendix A:
OQI
: Office for Quality Improvement
(Source:
http://www.wiscinfo.wisc.edu/improve/)
University of Wisconsin- Madison, Bascom
Hall, 500 Lincoln Drive, Madison, Wl 53706-1380-USA
tel: (608)262-6843, fax: (608)263-2081,
email:quality@mail.bascom.wisc.odu.
back to Contents
Appendix B:
CQPI
: Center for Quality & Productivity Improvement
(Source:
http://www.engr.wisc.edu/centers/cqpi/)
10 Walnut Street, 575 WARF Building, Madison,
Wisconsin 53705
Telephone: (608) 263-2520 Fax: (608) 263-1425 E-mail:
quality@engr.wisc.edu
back to Contents
Appendix C:
The 14 points of Deming’s quality management
(read and see :
Deming WE,1989, Out of the Crisis, Ed. Massachusetts Institute
of Technology, Center for Advanced Engineering Study, Seventh
Printing, April, p 507, ISBN 0-911379-01-0
Deming WE, 1994, The new economics, for Industry,
Government, Education, Ed. Massachusetts Institute of Technology,
Center for Advanced Engineering Study, Second Edition)
back to Contents
Appendix D:
Quality Web Sites
TQM web sites:
Seven
Management (New)
Tools
Hoshin
Overview & History
Juran
DEMING's websites:
Bay
Area Deming Users Group
British
Deming Association
Dallas
Study Group
Deming
Cooperative
Deming
Electronic Network Web Site
French
Deming Association
John
Hunter's Deming links
Indiana
Quality, Productivity, Involvement Council
Madison
Area Quality Improvement Network
MIT/CAES
Deming site
Ohio
Quality and Productivity Forum
Russian
Deming Association
The
W. Edwards Deming Institute
KAIZEN websites:
Kaizen
Institute
Kaizen
from the Persp. of Comp. Advantage
Quality
Digest
back to Contents
Quality, Higher Education and Research Web
Sites
UW-Madison
UW-Hospitals & Clinics
UW-Office
of Quality Improvement
UW-Center
for Qual. & Produc. Improvement
UW-Research
& Sponsored Programs
UW-Research
Park
UW-WARF
(Alumni Foundation)
UW-University-Industry
Relations
UW-Teaching
Academy
UW-Creat. Coll. Acad. Envir. (CCAE)
UW-Graduate
School
American Association of Higher Education
National
Science Foundation
WebCT
back to Contents
Quality, Health, Biomedical Clinical &
Engineering Web Sites
Association
for the Advancement of Medical Instrumentation
(AAMI)
American
Association of Physicists in Medicine
(AAPM)
American
College of Clinical Engineering (ACCE)
American
College of Medical Physics (ACMP)
American
College of Radiology (ACR)
American
National Standards Institute (ANSI)
American
Society for Healthcare Engineering
(ASHE)
American
Society for Quality (ASQ)
Baldrige
Criteria for Performance
Excellence
Biomedical Engineering
Department (BME UW Madison)
Emergency
Care Research Institute
(ECRI)
Engineering
in Medicine and Biology Society
(EMBS)
International
Federation for Medical and Biological Engineering
(IFMBE)
International
Organization for Medical Physics
(IOMP)
International
Society for Measurement & Control (ISA)
International
Society for Quality in Healthcare (ISQua)
Intern.
Union for Physical and Eng. Sciences in Medicine
(IUPESM)
Joint
Commission on Accreditation of Healthcare Organizations
(JCAHO)
National
Fire Protection Association (NFPA)
National
Institutes of Health (NIH)
National
Institute of Standards and Technology
(NIST)
Nuclear
Regulatory Commission (NRC)
University
HealthSystem Consortium
(UHC)
French websites :
Agence
Nationale d’Accréditation et d’Evaluation en
Santé (ANAES)
Association
Française des Ingénieurs Biomédicaux
(AFIB)
Association des Agents de
Maintenance Biomédicale (AAMB)
Portail Biomédical Hospitalier
back to Contents
- 1
Ordonancy of 24 April1996.
- 2
http://www.utc.fr/~farges/Qualite/Q_formation/Q_formation.html
- 3 UE
common position of 24 September1998 (Farnleitner,
98/561/EC)
- 4 http://www.wisc.edu/
- 5 http://www.greatermadisonchamber.com/move/pop2.htm
- 6 http://www.entrepreneur.com
- 7 http://www.wiscinfo.wisc.edu/improve/
- 8
http://www.wiscinfo.wisc.edu/improve/
- 9
see Appendix
A
- 10
http://www.wiscinfo.wisc.edu/improve/who/newsletter.html
- 11
see Appendix
B
- 12
Wisconsin
Alumni Research Foundation :
http://www.wisc.edu/warf/
- 13
http://www.engr.wisc.edu/centers/cqpi/short_list.htm
- 14 http://www.engr.wisc.edu/consortia/qasrc/
- 15
http://www.maqin.org/
- 16 http://wiscinfo.doit.wisc.edu/teaching-academy/
- 17 http://wiscinfo.doit.wisc.edu/teaching-academy/beingnew.html
- 18 http://wiscinfo.doit.wisc.edu/teaching-academy/itwhitepaper.html
- 19 http://www.aahe.org/
- 20 http://www.wisc.edu/MOO/
- 21 http://wiscinfo.doit.wisc.edu/teaching-academy/teaching_ideas_network.html
- 22 http://www.wisc.edu/ccae/
back to
Contents
- 23 http://www.wisc.edu/ccae/ccle/index.html
- 24 http://www.wisc.edu/ccae/MOO/
- 25 http://www.rsp.wisc.edu/
- 26 http://www.rsp.wisc.edu/chap2/rr32.html
- 27 http://www.rsp.wisc.edu/services/guides.html
- 28
http://www.engr.wisc.edu/bme/
- 29 http://www.whitaker.org/
- 30
http://www.cs.virginia.edu/research/sponsors.html#foundations
- 31 http://www.cs.virginia.edu/~robins/
- 32
http://www.uwhospital.hosp.wisc.edu/
- 33
http://www.jcaho.org
- 34
http://kermaosf.medphysics.wisc.edu/
- 35
http://www.uhc.edu
- 36 JCAHO,
1998, The Environment of Care® Handbook, Ed JCAHO, 129
pages, ISBN: 0-86688-589-7
- 37 http://www.aami.org/
- 38 http://www.ansi.org/
- 39 http://www.afnor.fr
- 40 http://www.nfpa.org
- 41 Grant
asked to the French Research Ministry (April 2000)
- 42
International standards about Quality System
(version 1994 : 9001, 9002, 9003 ; version 2000 :
9001)
- 43
European standards series about accreditation
of trial and measure laboratories
- 44
Ordonancy of April, 24, 1996
back to
Contents